Posts tagged ‘intestines’
Talking About the Hard Stuff
Today’s post is going to be pretty heavy- I am exploring some of the hard stuff (no not alcohol) that we IBD patients and advocates don’t like to talk about.
Most days, I don’t think about how serious Crohn’s disease and ulcerative colitis can be. I see my husband who, after a few rough years, is living a relatively normal life with little pain. Yes, he still frequents the bathroom and yes he still has cramping but compared to previously, his life has changed for the better.
That’s not the case for many people. This past year has been a rough one for several of my IBD friends. In July, one had her temporary ileostomy made permanent after spending a month in the hospital with uncontrollable inflammation and being under the impression that it was going to be reversed. Another had the last several inches of her colon removed two days after doing a half-marathon and has been struggling with issues at her surgery site. A third has been in and out of the hospital over the past few months with partial blockages.
If you live with a mild to moderate form of IBD, you often aren’t faced with the severity of the disease – in some cases, it can be fatal. This morning, I woke up to find out that a member of one of the IBD Facebook groups I belong to passed away due to complications of her disease. I don’t know the full details of her death but I was told that she had a stricture and trouble breathing, called 9-1-1, and by the time the ambulance arrived, she had passed away. She leaves behind two small children and her husband.

Prior to her death, the only one I had heard of was Jennifer Jaff, who passed away in 2012 from Crohn’s disease complications.
More often than not, IBD patients experience complications from their disease. If not detected and treated early, some of these complications can be extremely harmful and in rare instances, cause death.
(more…)
Guest Post: The Silent Battle Before an Ostomy
Today’s post comes from Brian Greenberg, the man behind the Intense Intestine’s Foundation. Brian has battled Crohn’s disease for years and, two-and-a-half years ago, became an ostomate. Despite having an ileostomy, Brian refuses to let his disease get in the way of his love for the outdoors and life. Below he talks about the internal struggle many patients go through prior to getting an ostomy.

Transplant for patients with severe Crohn’s?
Over the past few months, I’ve written posts about all sorts of new treatments being studied for IBD- bone marrow transplants and whipworms to name a few. Those sounded a little crazy to me but definitely intriguing. However, a new study published by the University of Pittsburgh Medical Center suggests that intestinal or multivisceral (three or more abdominal organs) transplants are effective treatments for patients with Crohn’s so severe that they no longer tolerate an IV nutrition.
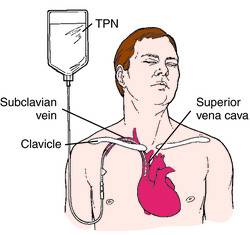
As we all know, when Crohn’s is severe, its hard to absorb nutrients or even eat. For those who have irreversible intestinal failure, they may need to receive nutrition through a tube intravenously, known as total perenteral nutrition. According to the study, those who do not tolerate the IV nutrition are often referred for an intestinal transplant.
The ABC’s of Crohn’s & UC: “J” & “K”
It’s been a few weeks since I did an installation in my ABC’s of Crohn’s & UC series. With other topics arising and Crohn’s & Colitis Awareness Week occurring, it’s fallen off my radar. So here is the next installation, and it will be a short one: J and K.

Jejunoileitis: One of the types of Crohn’s Disease. Jejunoileitis affects the jejunum (see below). Symptoms include cramps after meals, fistulas, diarrhea, and abdominal pain. Kind of sounds like all the other types of Crohn’s.
Jejunum: The upper half of the small intestines.

J-Pouch: One name for an ileo-anal pouch. The J-Pouch is an internal reservoir where the rectum would be. A J-Pouch is traditionally done through a multi-part surgery. The first surgery involves the removal of the large intestines and rectum and the fashioning of the pouch. At the end of the first surgery, the patient is given a temporary ileostomy in order to give the pouch time to heal. After a period of time (typically 6-12 weeks), a second surgery is performed known as the “take down” in which the ileostomy is reversed.

Kidney Stones: One of the most common kidney complications in Crohn’s patients. According to CCFA, kidney stones are common in patients who has Crohn’s in the small intestines because of fat malabsorption. You are at a higher risk for kidney stones if you’ve had a number of bowel resections because you are more prone to dehydration. Symptoms of kidney stones include sharp pain (particularly in your lower back), nausea, vomiting, and blood in the urine. Treatment calls for an increased fluid intake and a diet that is rich in juices and vegetables. If you are unable to pass the kidney stones on your own, you may have to have them removed which is through a simple procedure.

Kock Pouch: A Kock Pouch is an internal pouch formed by the terminal ileum after a colectomy. The pouch has a large volume so that feces can be stored temporarily without the need for a stoma bag. A Kock Pouch may be created if the patient cannot have an ileo-anal pouch or who develop incontinence after an ileo-anal pouch.
